.

พล.ต. หญิง รศ. พญ. อภัสนี บุญญาวรกุล
แผนกต่อมไร้ท่อ กองอายุรกรรม
โรงพยาบาลพระมงกุฎเกล้า
ข้อมูลของยา CagriSema และ Preexisting Diabetes and Pregnancy
CagriSema in type 2 diabetes
Semaglutide เป็น glucagon-like peptide 1 (GLP-1) agonist ฉีดใต้ผิวหนังสัปดาห์ละครั้ง ได้รับการอนุมัติให้ใช้ในการลดน้ำหนัก การศึกษาใน phase 3 ระยะเวลา 68 สัปดาห์ ในผู้ใหญ่ที่น้ำหนักเกินหรือโรคอ้วน และในโรคเบาหวานชนิดที่ 2 การให้ Semaglutide (ขนาด 2.4 มิลลิกรัม) ลดน้ำหนักเฉลี่ยได้ 9.6 %
Cagrilintide เป็น long-acting amylin analogue จับกับ calcitonin receptor และ amylin receptors พบว่าลดการรับประทานอาหาร และลดน้ำหนัก ดังนั้นการใช้ fixed-dose combination ของ cagrilintide และ semaglutide (CagriSema) ได้รับการประเมินในการลดน้ำหนัก และการควบคุมน้ำตาลในเลือด โดยผลการศึกษาคาดว่าจะได้ผลดีกว่าการใช้ semaglutide หรือ cagrilintide เพียงชนิดเดียว
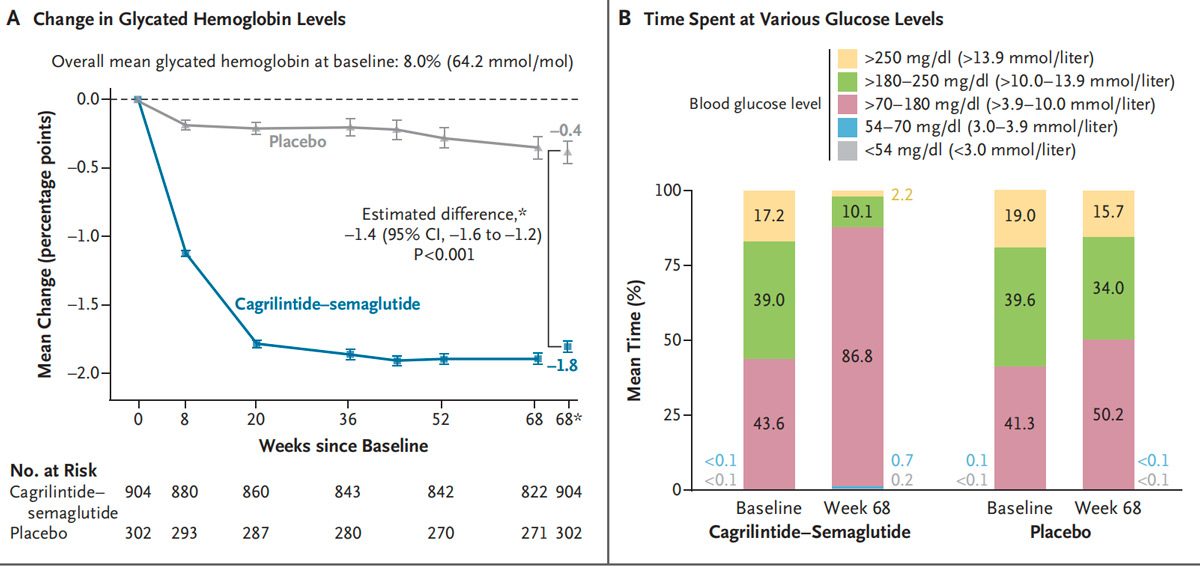
REDEFINE 2 เป็นการศึกษาในผู้ใหญ่ที่น้ำหนักเกิน หรือ อ้วนและเป็นโรคเบาหวานชนิดที่ 2 เพื่อประเมิน efficacy และ safety ของการใช้ cagrilintide-semaglutide (ในขนาด 2.4 มิลลิกรัมของแต่ละชนิด) เปรียบเทียบกับ placebo โดยมีการให้ lifestyle interventions ในผู้เข้าร่วมวิจัยทั้งสองกลุ่ม ร่วมกับมี subgroup ของผู้เข้าร่วมวิจัยที่มีการใช้ continuous glucose monitoring ผู้เข้าร่วมวิจัยได้ cagrilintide-semaglutide (904 ราย) ได้ placebo (302 ราย) อายุเฉลี่ย 56.0 ปี เพศชาย 52.8%
น้ำหนักเฉลี่ย 102.2 กิโลกรัม ค่า glycated hemoglobin level 8.0% มีการติด continuous glucose monitoring 16.5% ใน cagrilintide-semaglutide และ 16.6% ใน placebo ผลการศึกษา treatment-policy estimand ค่าเฉลี่ยน้ำหนักลดลง 13.7%
ที่ 68 สัปดาห์ ส่วน trial-product estimand ค่าเฉลี่ยน้ำหนักลดลง 15.7% และ placebo ลดลง 3.1% มีการลดลงของ glycated hemoglobin level –1.8 เทียบกับ placebo –0.4
อ่านรายละเอียดเพิ่มเติมจาก N Engl J Med 2025;393:648-59
Reference: Davies MJ, Bajaj HS, Broholm C, Eliasen A, and Garvey T, et al. Cagrilintide–Semaglutide in Adults with Overweight or Obesity and Type 2 Diabetes. N Engl J Med 2025;393:648-59
Preexisting Diabetes and Pregnancy: An Endocrine Society and European Society of Endocrinology Joint Clinical Practice Guideline
ผู้ป่วยเบาหวานทั้งชนิดที่ 1 และ ชนิดที่ 2 เพิ่มความเสี่ยงต่อการเกิดภาวะแทรกซ้อนทั้งในมารดาและบุตร ดังนั้น Endocrine Society และ European Society of Endocrinology ได้เขียนคำแนะนำเกี่ยวกับการตั้งครรภ์ สรุปบางประเด็นดังนี้
Recommendation 1: In individuals with diabetes mellitus who have the possibility of becoming pregnant, we suggest asking a screening question about pregnancy intention at every reproductive, diabetes, and primary care visit. Screening for pregnancy intent should also be addressed at urgent care/emergency room visits when clinically appropriate (2 | ⊕OOO).
Recommendation 2: In individuals with diabetes mellitus who have the possibility of becoming pregnant, we suggest use of contraception when pregnancy is not desired (2 | ⊕⊕OO).
Recommendation 3: In individuals with type 2 diabetes, we suggest discontinuation of glucagon-like peptide-1 receptor agonist (GLP-1RA) before conception rather than discontinuation between the start of pregnancy and the end of the first trimester (2 | ⊕OOO).
Recommendation 4: In pregnant individuals with type 2 diabetes mellitus (T2DM) already on insulin, we suggest against routine addition of metformin (2 | ⊕OOO).
Recommendation 5: In individuals with preexisting diabetes mellitus (PDM), we suggest either a carbohydrate-restricted diet (175 g per day) or usual diet (>175 g per day) during pregnancy (2 | ⊕OOO).
Recommendation 6: In pregnant individuals with type 2 diabetes mellitus (T2DM), we suggest either continuous glucose monitor (CGM) or self-monitoring of blood glucose (SMBG) (2 | ⊕OOO).
Recommendation 7: In individuals with preexisting diabetes mellitus (PDM) using a continuous glucose monitor (CGM), we suggest against the use of single 24-hour CGM target < 140 mg/dL in place of standard-of-care pregnancy glucose targets of fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL, 2-hour postprandial < 120 mg/dL (2 | ⊕OOO)
Recommendation 8: In individuals with T1DM who are pregnant, we suggest the use of a hybrid closed-loop pump (pump adjusting automatically based on CGM) rather than an insulin pump with CGM (without an algorithm) or multiple daily insulin injections with CGM (2 | ⊕OOO).
Recommendation 9: In individuals with PDM, we suggest early delivery based on risk assessment rather than expectant management (2 | ⊕OOO).
Recommendation 10: In individuals with PDM (including those with pregnancy loss or termination), we suggest postpartum endocrine care (diabetes management), in addition to usual obstetric care (2 | ⊕OOO).
Contraception and Diabetes Mellitus
ผู้ป่วยเบาหวานควรมีการควบคุมระดับน้ำตาลในเลือดให้เหมาะสม ร่วมกับการตรวจภาวะแทรกซ้อนของเบาหวาน ก่อนการตั้งครรภ์ ดังนั้นการวางแผนในการคุมกำเนิดมีความสำคัญ
New antidiabetic medication: any effect on fertility ?
ยาในกลุ่ม glucagon-like peptide -1 receptor agonists (GLP-1 RAs): oral semaglutide ไม่ส่งผลต่อระดับยาคุมกำเนิด ethinylestradiol/ levonorgestrel ส่วน semaglutide ชนิดฉีด ผลต่อยาคุมกำเนิดยังไม่ชัดเจน อย่างไรก็ตามมีรายงานการตั้งครรภ์ในผู้ที่ใช้ semaglutide ทั้งที่ใช้ยาคุมกำเนิดร่วมด้วย “Ozempic babies” ในการวิจัย Experimental data พบว่า GLP-1 มีผลเพิ่ม preovulatory LH peak
Dulaglutide มีผลลด Cmax ของ ethinylestradiol ลดลง 13% และ norelgestromin ลดลง 26% ,
Liraglutide มีผล ethinyl estradiol และ levonorgestrel concentrations ลดลง 12% และ 13% ,
Tirzepatide มีผลลด AUC ratios ลดลง 20% ของ ethinyle stradiol, 21% ของ norelgestromin, Cmax ของ ethinylestradiol ลดลง 59%, และของ norelgestromin ลดลง 66 % การได้ Tirzepatide ทำให้ delay in the maximum plasma concentration time 2.5 to 4.5 h ดังนั้น ในผู้ที่ได้ยา tirzepatide ควรเพิ่มขนาดยา oral contraceptives
ยากลุ่ม sodium-glucose transport proteins 2 inhibitor (SGLT-2i) มีการศึกษาของยา canagliflozin ร่วมกับ oral contraceptive จะเพิ่ม Cmax 22 % และ AUC 6 % ของยา oral contraceptive
Use of contraception in diabetes mellitus: what to choose
การใช้ subcutaneous progestin implants (etonogestrel หรือ levonorgestrel) และการใช้ intrauterine devices (copper, levonorgestrel-releasing) เป็นวิธีที่มีประสิทธิภาพในการคุมกำเนิด
ยาคุมกำเนิดที่มี estrogen/ progesterone มีข้อมูลเพิ่ม prediabetes (odds ratio [OR]: 2.0, 95% CI: 1.3-3.2) และ T2 diabetes (OR: 3.3, 95% CI: 1.1-9.7) การได้ยานานเกิน 5 ปี เพิ่มความเสี่ยงต่อการเกิด prediabetes 2.2 เท่า (95% CI: 1.3-3.7) และ ความเสี่ยงต่อการเกิดเบาหวาน 4.5 เท่า (95% CI: 1.5-13.5) ในผู้ที่เป็นเบาหวานและ BMI > 35 kg/m2 มีความเสี่ยงต่อการเกิด deep vein thrombosis และ thromboembolism ไม่ควรเลือกใช้ยา combined oral contraception
- Wyckoff JA, Lapolla A, Asias-Dinh BD, Barbour LA, Brown FM, et al. Preexisting Diabetes and Pregnancy: An Endocrine Society and European Society of Endocrinology Joint Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 2025, 110, 2405–2452
- Panou T, Gouveri E, Gerede A, Tsikouras P, and Papazoglou D, Contraception and Diabetes Mellitus. Exp Clin Endocrinol Diabetes 2025; 133: 268–277
งานประชุมสาขาต่อมไร้ท่อที่น่าสนใจ เดือน ก.ย. – ธ.ค. 2568.

• American Thyroid Association Annual Meeting | 10 – 14 September 2025 Scottsdale – AZ, USA

• The 9th Asian Federation of Osteoporosis Societies Congress 2025 & The 20th Thai Osteoporosis Foundation Annual Conference | 25 – 27 กันยายน 2568 ณ เมอเวนพิค บีดีเอ็มเอส เวลเนส รีสอร์ท กรุงเทพฯ


